
Although the rise of cancer immunotherapy may seem meteoric to many, the history goes back over 100 years to William B. Coley, often referred to as the father of immunotherapy.
In the 1890s, Dr. Coley recognized a correlation between patients with advanced cancer experiencing regression and a severe skin infection, erysipelas. Based on this observation, he used live bacteria to treat patients with inoperable sarcoma or carcinoma1. In addition, in 1909 Paul Ehrlich proposed the cancer immune surveillance hypothesis, which states that cancer arises spontaneously, and the immune system can recognize it and repress growth of tumors2.
However, only in the last few years has immunotherapy become a cornerstone of cancer treatment. This is due in large part to the success of PD-1/PD-L1 blockade, which is able to cause long-term remission with limited associated immune-related adverse events (irAEs). This is in contrast to previous immunotherapy attempts, such as IL-2 therapy, which proved too toxic at doses required to achieve tumor regression. What’s the difference? PD-1/PD-L1 blockade inhibits an immune evasion strategy specific to the tumor, while an approach like high dose IL-2 aims to generally enhance immune activation3. Unfortunately, only a small percentage of patients respond to PD-1/PD-L1 blockade. This low response rate is likely the result of additional immune evasion strategies employed by tumors.
A successful response to PD-1/PD-L1 blockade requires the presence of T cells that can detect the tumor and are capable of effector functions such as cytotoxicity. Those T cells need to be activated by dendritic cells capable of antigen presentation. However, both T cells and dendritic cells can be actively excluded from the tumor4. Even if T cells were successfully activated, they often co-express other inhibitory receptors such as TIM-3 and Lag3, and as a result, PD-1/PD-L1 blockade alone may not be sufficient to restore effector function5. Finally, the tumor microenvironment needs to be permissible to T cell activation, which is often not the case due to the presence of immunosuppressive molecules and cell types such as regulatory T cells, myeloid-derived suppressor cells, and suppressive “M2-like” macrophages.
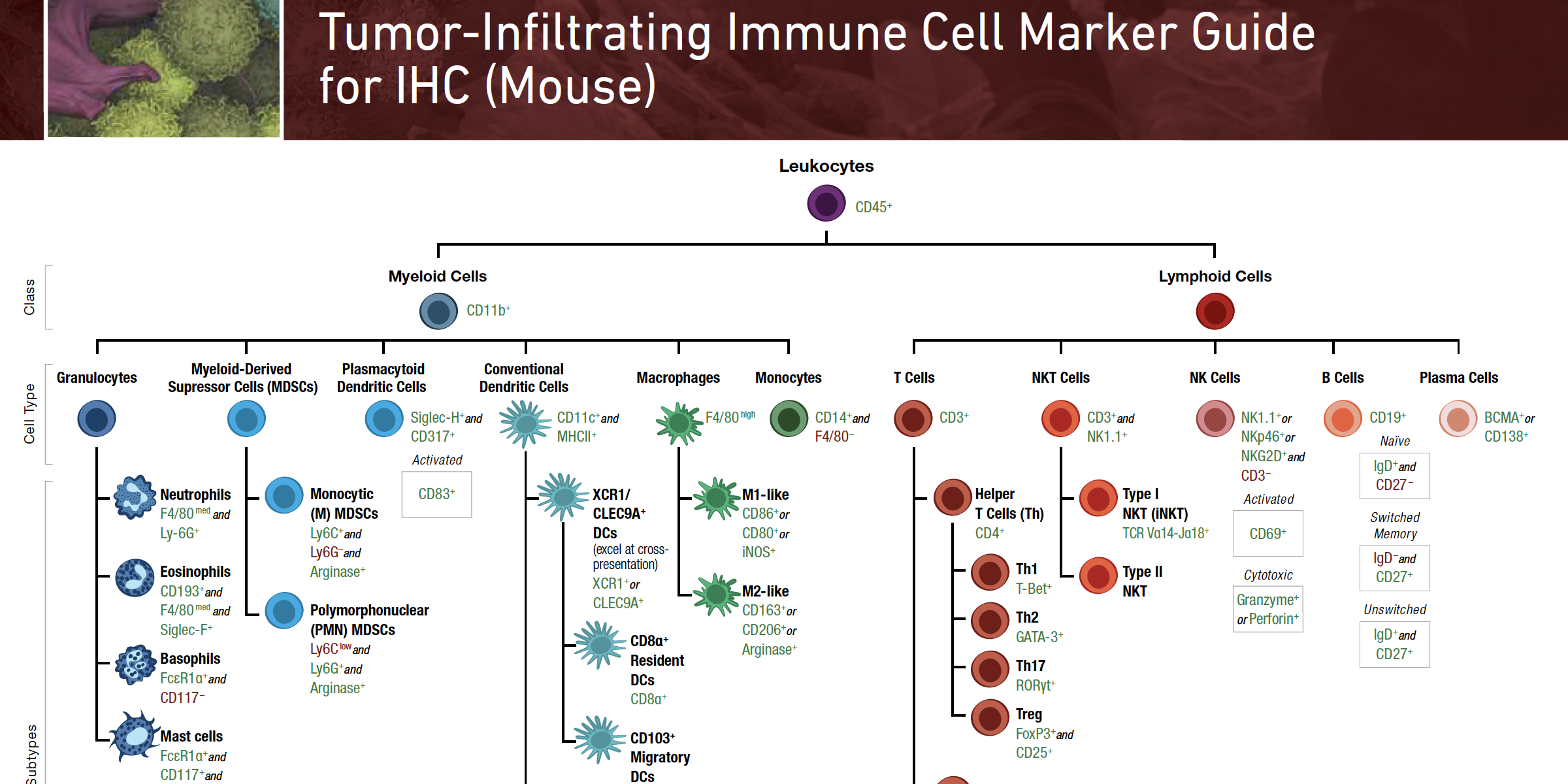
Dramatically increasing the success of cancer immunotherapy while limiting irAEs will likely require an understanding of exactly which immunosuppressive mechanisms are at play in each individual tumor. One way to obtain this information is to understand the phenotype and function of immune cells in the tumor. To assist researchers exploring this field, we created a phenotyping guide for identifying the immune cells known thus far to be most influential in the tumor immune response. Examples include CD8 T cells, dendritic cells that excel in antigen presentation to CD8 T cells (cross-presentation), and immunosuppressive cell types described above. We’ve also included markers that can be used to infer function of these cells. The combination of immune cell phenotype and function can be applied to understand which immunosuppressive mechanisms may be preventing a successful tumor immune response and therefore could represent the opportunities for effective therapeutic intervention.
While immune phenotyping by flow cytometry has been a mainstay of immunology for decades, tumor immunology necessitates immune phenotyping by IHC. FFPE tumor tissue is often the most accessible sample type and observation of spatial relationships between cells in the tumor provides valuable information for understanding the tumor immune response. Therefore, we created this first set of guides from the perspective of observing immune cells in intact tumor tissue. Given the technical constraints of multiplex IHC, we aimed to provide the minimum set of most well-established markers enabling identification of each cell type. Stay tuned for future flow-cytometry-specific versions of the Immune Cell Marker Guide.
Download the Immune Cell Marker Guide for IHC
References:

